Skip to content
Facebook
Twitter
Yelp
Google
Home
Who We Are
Find the best back pain doctor in NYC!
Learn More About Us
About
Meet the Doctor
Blog
Contact Us
(646) 665-7109
PHYSICAL THERAPY
Are you looking for
Physical Therapy?
Pilates
Therapeutic Massage
Spinal Decompression
Modalities
Scoliosis Rehabilitation
Therapeutic Yoga
Therapeutic Exercises
Vestibular Rehabilitation
Temporomandibular Joint (TMJ) Therapy
PAIN MANAGEMENT
Physical Medicine & Rehabilitation / Physiatry
Orthopedic Medicine
Sports Medicine Services
Nerve Blocks or Injections
Trigger Point Injections
Epidural
Acupuncture
CHIROPRACTIC
THE DIVERSIFIED TECHNIQUE
SPINAL MANIPULATION (aka Spinal Mobilization)
THE ACTIVATOR METHOD
SOFT TISSUE MOBILIZATION
EXTRA SPINAL MANIPULATION
NEUROMUSCULAR RE-EDUCATION
CONDITIONS
Ankle & Foot Pain
Back Pain
Elbow Pain
Hip Pain
Knee Pain
Neck Pain
Shoulder Pain
Wrist/Hand Pain
Home
Who We Are
Find the best back pain doctor in NYC!
Learn More About Us
About
Meet the Doctor
Blog
Contact Us
Physical Therapy
Pilates
Therapeutic Massage
Spinal Decompression
Modalities
Scoliosis Rehabilitation
Therapeutic Yoga
Therapeutic Exercises
Vestibular Rehabilitation Therapy
Temporomandibular Joint (TMJ) Therapy
Pain Management
Physical Medicine & Rehabilitation / Physiatry
Orthopedic Medicine
Sports Medicine
Nerve Blocks or Injections
Trigger Point Injections
Epidural Steroid Injections
Acupuncture
Chiropractic
Diversified Technique
Spinal Manipulation
Activator Method
Soft tissue mobilization
Extra spinal manipulation
Neuromuscular
Conditions
Ankle and Foot Pain
Back Pain
Elbow Pain
Hip Pain
Knee Pain
Neck Pain
Shoulder Pain
Wrist and Hand Pain
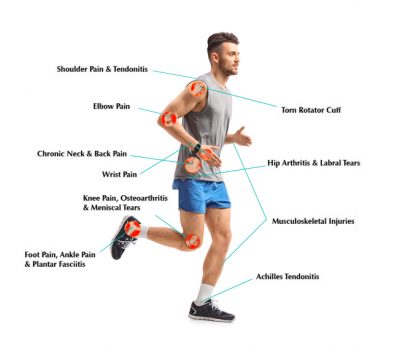
Tell the Doctor Where It Hurts:
CONTACT US
BOOK ONLINE
Tell the Doctor Where It Hurts:
Steven Moalemi
2021-08-05T22:45:51-04:00
New Patient Form
Error:
Contact form not found.
Page load link
Go to Top